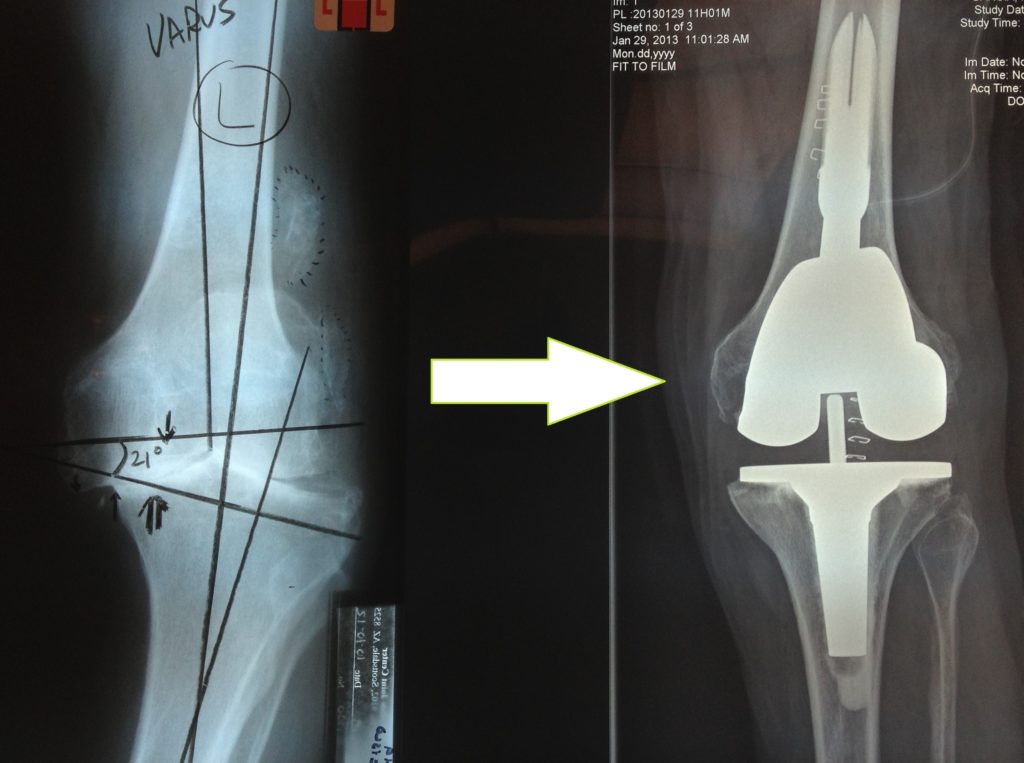
Some knees are more severely involved with arthritis than others. The knee shown in the picture below shows bone on bone grinding in more than one compartment. These knees are best treated with a full or “total” knee replacement which replaces both sides of the knee with metal and plastic surfaces, as well as the knee cap /femur joint which gets a plastic button. This knee demonstrates varus ( or bowed-leg ) deformity, along with subluxation because of loss of ligament stability. Different orthopedic surgeons will use different brands of total knee implants. There are many good choices available and you should talk to your surgeon about why he likes to use the knee that he uses.
New Technology in Total Knee Arthroplasty
Newer and better designed total knee implants are becoming available for patients. More bio-compatible materials coupled with computer assisted designs are allowing better “fitting” to most patients at the time of surgery. Modern Total Knee systems now have some particularly positive updates in design. I like the more natural shaped implants that “fit” more sizes of femurs – and which also improves patella tracking. Modern Polyethylene components will resist oxidative degradation and wear over time better. Different surgeons choose which knee replacement design they are most satisfied with. It is good for patients to learn more about the actual implant choices, and ask their surgeon what they like to use and why!
Total Knee Replacement Expectations
Total Knee Replacement Expectations:
This is an important blog topic on total knee replacement to be aware of. While most patients are ultimately satisfied with their new knees, our AAOS academy has done survey studies that show that 10 to 20% of all total knee patients feel their total knee replacement did not “meet their high expectations” for function.
Starting a total knee.
Patients tend to expect “perfection” including unlimited range of motion and pain-free function. This doesnt mean that their knees are failures, just that their initial expectations were too high. Many patients do have some discomfort after having total knees. Artificial knee “machines” have moving parts and are subjected to very high weight bearing and activity stress. Some patient’s expectations of what their future total knee can do is not always accurate. This is particulary evident in the younger group of patients (age 40-60) who expect to participate in sports and heavier work activities.
Jay Buchtel shows off his excellent range of motion after total knee replacement
It is natural for patients to be optimistic, particularly with the increase in consumer marketing associated with total knee products. Sometimes, after years of chronic pain, patients have built up expectations that their new knee will be a miracle cure with zero drawbacks. While still the best procedure option to reduce chronic disability and pain from bone on bone arthritis in many patients, there are no quarantees of complete success. Many knees will still swell a little with overactivity, and it can take over two years for full healing of the soft tissues around a total knee. This includes full healing of the collateral ligaments. We also see range of motion gains in some patients for up to two years after surgery.
Happy total knee patients really make my day!
If you are younger, you must understand that all total knees may eventually fail after years of function and need to be revised. It is also possible that your range of motion of your total knee may not be as good as your opposite knee. This is because it is not always possible to get both full stability of the knee, and also full range of motion. (One of those “can’t eat your cake and have it too” situations. ) The patella (kneecap) is an extremely “sensitive” bone, and the number one source of anterior pains around the total knee. Sitting with the knee flexed, and certainly kneeling down, puts pressure on the kneecap that can be uncomfortable at times. There may be no effective treatment for this except activity modification and muscle strengthening. Most patients do feel that their new knee is “better” than their old worn out knee, but you should expect there will still be some aches and pains, associated with certain activities, even after your total knee. You will know when it is time to have total knee surgery, based on how disabled you are when you make the decision to proceed. Most patients will have tried many non-surgical options before proceeding with total knee replacement. It is a good operation for appropriate candidates with bone on bone grinding.
Total Knee Arthroplasty
Total knee arthroplasty is another term for total knee replacement. Arthro means joint in Latin, and plasty means to mold or create ( a new joint). The results of total knee arthroplasty are getting better with new materials and techniques. I happen to favor a rotating platform type of design. I think it adds a shock absorber function to the artificial joint. Many of my patients go back to playing softball and tennis with their knee replacements. I do ask that they choose not to do long distance running or jogging as I think this may eventually damage the cement bond to the bone. There is no research data on how much sports or activity is acceptable. It all comes down to common sense. Bike riding and swimming during the summer is particularly helpful in keeping the artificial joint mobile. You can do yoga and stretching exercises every day. Using the knee does help to keep it more functional. Gliding sports and activities are better than pounding and jumping activities. Strong muscles make for a more stable and satisfying total knee arthroplasty. If your knee pain is severe, you should come in for an evaluation. Call our main number at The Scottsdale Joint Center at 480-994-1149 . We will show you models of the different types of total knee arthroplasty that are now available.
Robots, Computer Navigation, and Custom Cutting Blocks In Knee Replacement?
As imperfect human beings, we are always looking for a way that technology can make us more accurate at what we do. Total knee replacement technology is no different. Unfortunately, every individual and every knee has its own unique “personality” that does not lend itself well to generalized solutions. After working with computer navigation which was the “next big advance” about 10 years ago, we were all disappointed that the overall results of knee replacement were not improved, and in some studies were made worse. We also went through the “phase” of tiny incision “minimally invasive” knee arthroplasty. Results in this group were definitely worse. Part of the reason is the knee has to be perfectly “balanced” through an infinite range of motions and positions. Not just flexion and extension from 0 to 135 degrees, but a variety of rotational positions and “varus-valgus” positions ( side tilt in either direction ). Our computers also can only give us out information based on the “input data” we program into it. If you use “eye-sight” points of information, you will get errors entered into the computer that can easily add up to a worse result than a “free-hand” arthroplasty. It turns out that a trained knee surgeon, after years of practice, has developed a very accurate computer in his (or her) brain. When an external computer is available that is better than my brain, I will switch to it!
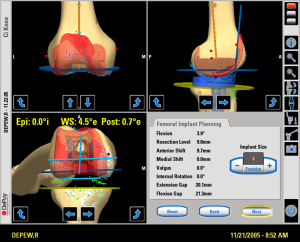
Computer navigation screen for total knee replacement.
Pre-operative CTT scans and MRIs give the computer data in only one knee position! How can the computer know what directions to give the surgeon to make a bone cut in a different position, for instance 90 degrees opposed. It “estimates” based on a data base collected from human volunteers. Also, the computer can not fathom the elasticity, or stretch, in any one person’s ligaments. Since ligament tension is also dependent on the amount of knee flexion, even perfectly directed “bone cuts” can end up with an unstable knee at times because the ligaments must also be under equal tension in all positions. Very hard to accomplish! This is why most high volume total knee surgeons use the “feel” of the knee in their hands as the input to the “computer” in their brains. We “trial” a number of different implant positions and sizes until we get the best and most balanced knee.
Dr. Kozinn with an early version of the Total Knee computer.
The “robots” that are coming out are not better. They have been used for their “marketing value”, as it is natural to assume a robot or computer is “smarter” than a human. Most of the computers out there now still require a human to “manually over-ride” as soon as it is clear that the “pre-set” plan generated from a uni-position CTT or MRI is not going to work out in the real world. A number of research studies have now shown that the surgeon will “abandon” the computerized plan, or revise the cuts yielded from customized cutting blocks up to 70% of the time they are used. Wow! There is also an additional expense and inconvenience of getting these special scans pre-op. I call these custom cutting block operations “total knees by numbers”, analogous to the childhood art game of “paint by numbers”. If you survey most of the high volume fellowship trained total knee surgeons in practice right now, you will find that most do not utilize these devices. When these technologies are really better for patients, we will use them. Right now, it is best to choose an experienced surgeon and not the best robot!
Stuart C. Kozinn MD
Chief of Surgery, HonorHealth Osborn
www.scottsdalejointcenter.com
Total Knee Recovery
TOTAL KNEE RECOVERY:
Total knee recovery is very much related to the control of your pain. I use a muscle sparing approach to knee replacement that minimizes cutting of the quadriceps tendon, allowing for a faster total knee recovery. Depending on the size of the patient’s thigh, more or less “release” is required to move the patella (kneecap) out of the way, so that the metal implants can be inserted. I don’t think the term “minimally invasive” is an accurate way to describe total knee replacement surgery. There is nothing minimal about removing bone from the surface of the femur and the top surface of the tibia. The length of the skin incision, while a definite cosmetic concern, is not really relevant from a functional recovery standpoint. Paradoxically, a longer skin incision most often allows us to move the muscles over without cutting them, much like “spreading curtains”, to gain access to the bone ends.
We can do our partial knee replacements with smaller incisions without cutinng the quadriceps muscle, which leads to a faster recovery.
(BTW: Our muscle sparing anterior hip replacement operations are similar, in that we can implant the prosthesis without cutting any muscles at all, as long as we can spread the longitudinal muscles apart -the interval between rectus femoris and tensor fascia latta). So how do we control pain? I am glad you asked!
Our pain management protocol is multimodal, meaning we use different modalities working on different pain pathways to add up to excellent pain relief without side effects. In the “old way”, a patient may have received a general anesthetic and IV narcotic therapy. This leads to a sudden surge of severe pain when the anesthesia is terminated. Narcotics have various negative side effects: Lethargy, respiratory depression, nausea, vomiting, sick feeling, confusion, anxiety, itching and constipation to name a few. Instead, we use a regional anesthetic ( spinal or epidural) which completely removes all pain until it gradually wears off. The gradual wearing off is a key component, in that our human brains better accommodate to pain in a gradual way, allowing us to respond by secreting our own endogenous “narcotic like” substances called endorphins and encephalin. During this time, and additional modality, a femoral nerve block, continues the pain blockade to about 70% of the knee (much like the dentist blocks the nerves in your gums with a “novacaine”shot.) The femoral nerve block, or a newer version called the “adductor canal block” is applied in the pre-op area by the anesthesiologist before the spinal is put in. The patient can still have as much IV sedation as is required to alleve anxiety. Some patients prefer to stay “awake” throughout the procedure, and often I have had conversations with patients during their painless surgeries! This technique is especially good in an elderly patient who is prone to confusion after receiving narcotics of sedatives.
the knee is encased in antibiotic impregnated steriele plastic to protect against skin bacteria entering the wound.
We also inject a potent local anesthestic called “Exparel”, which is a long acting “novacaine” type drug, in the skin and subcutaneous tissues to prolong the pain relief. This can have an effect up to 72 hours! As the spinal wears off in the recovery room, the patients are usually quite comfortable when I visit them before going up to their room. I often hear that “I have no pain:, but every patient going through total knee recovery is different. There is no question that we are all “wired” differently in regard to our tolerance and perception of pain. We also give medications, but slowly and gradually. We often add a “Celebrex” pill pre-op with a sip of water. We use IV “Tylenol” ( acetamenophin) pre-op as well. these medications are working in the background adding tot he multi-modality pain control.
Dr. Kozinn has been doing total knees for 28 years. here is one that followed up after 21 years and is doing great!
Our workhorse “drug” is IV Toradol, which is an aspirin like anti-inflammatory with super pain control ability. As long as there are no medical contraindications to its use (prior GI bleeding or Kidney failure), it is extraordinarly effective at controlling pain. With all of these techniques together, total knee recovery can be much more rapid. Early ambulation and mobility adds to the dynamics of pain control. When patients get out of bed early, they use positive mindset to decrease the perception of pain. We no longer use CPM machines as they keep patients strapped in bed. Range of motion is better when patients get up and walk an hour or two right after the surgery.
If you think you could benefit from a knee replacement, please come in to our office and have an evaluation. Total knee recovery is not as bad as it use to be.
Stuart C. Kozinn MD.
Dr. Kozinn was recently featured in the Camelback Corridor magazine.
Total Knee Replacement and Tennis
Many patients ask me if they can resume playing tennis after a total knee replacement. The answer is YES! I particularly like the function of a rotating platform total knee replacement in my tennis and racquet sport players. I have many successful athletes and weekend warriors out on the courts. In general, it is probably better to play doubles, as there is less running around over-all, but singles is also allowable. Obviously no guarantees can be made that ALL patients with a knee replacement will be able to play, but a very high percentage will. Most tennis players have waited “too long” to get their knees fixed, because of fear of having to give up their favorite past-time after surgery. It is better to have it done at a convenient time, as it is likely to be inevitable, and harder to recover after the deformity is very severe.
You can ride your mountain bike, and swim, and play tennis after your total knee ( just like Kary!)
Many patients need both total knee replacement “done” as there is a high proportion of hereditary or genetic based osteoarthritis of the knee affecting both sides. I suspect I will need my own total knee replacement in the future, and I will do my research and find the best surgeon I can to do it! I plan on playing lots of tennis, golf, ski-ing, wakeboarding, and swimming as I get older. If you have “worn out joints”, you should fix them and get back to an active life style. Sitting on the sidelines is not healthy!
The rotating platform total knee is my favorite for active people.
Total Knee Recovery at the Scottsdale Joint Center
Total knee recovery is getting much better these days. When I make rounds now the day after surgery, there are a lot more smiling faces. In the “old days”, the knees were very painful for a few days. Now we use new pain management techniques that minimize the pain without narcotics. We try to avoid general anesthetics that can lead to confusion and nausea post operatively.
Happy total knee patients really make my day!
First off, the spinal anesthesia allows a very gradual transmission of the pain to the brain- making it much more tolerable. We have the capacity to release our own narcotics ( endorphins) in response to stress, and the spinal makes this a better, more gradual process. Next, we use a femoral nerve block. Our specialist anesthesiologists are beginning to isolate the sensory component of the femoral nerve ( the saphenous branch), so that the pain is gone for 36+ hours, but the motor function stays intact. This will allow earlier and eventually same day discharge for motivated patients. We are also now using Exparel*, a timed release local anesthetic that can last up to 72 hours. By avoiding narcotics, patients are less nauseas, and are able to be more active. Toradol is a potent pain med that is not a narcotic, and we can inject this into the IV every 6-8 hours. Patients really are doing better, with a lot less pain.
Jay Buchtel shows off his excellent range of motion after total knee replacement
visit our webpage www.scottsdalejointcenter.com for more info on total joint replacements.
complex total knee replacement- It is ok to play tennis and golf after total knee replacement recovery!
How do you get the best total knee replacement you can?
Patients should do their research and should try to get the best total knee replacement they can. It always surprises me how many of my patients wait too long to fix their arthritic knees because they have heard that “total knees don’t last very long”. Actually, the results of knee replacements keep getting better over time. It isn’t really only about which device is used. I think a lot f it has to do with finding a surgeon who specializes in knee replacement. Studies have shown that higher volume total joint centers tend to have better results and less complications. You do need to do a little online research to find a qualified and experienced total knee surgeon. Look for a surgeon who has done an extra year of training called a “total joint replacement fellowship”. (PS: Dr. Kozinn did his joint replacement fellowship at Harvard Medical College at the Brigham and Women’s Hospital in Boston.)
Dr. Stuart Kozinn in his operating room at Scottsdale Osborn
Research suggests that approximately 85% of modern total knees will function well over 20 years ( assuming the patient survives that long). Patients are happier in the short term with new pain management techniques as well. The reasons for success are better materials, better implants, better techniques, better pain management, and better understanding of the rehab process needed. For instance, I have found that waiting a week before starting painful therapy exercises helps decrease initial bleeding and swelling and pain, and actually results in a faster recovery – possibly the opposite of what you might expect. In the end, the knee replacement surgery is a “controlled trauma”, and allowing for some initial healing goes a long way towards faster recovery. We also flex our knees over a pillow the first night of surgery. Some surgeons avoid this because they assume “it may make it harder to get the knee straight”. This is not true! The flexed knee is more comfortable, particularly when using a femoral nerve block to control pain, as it relaxes the posterior ligaments. It also has the added benefit of stopping any residual bleeding in the knee ( indirectly by tensing the soft tissues – the bleeding stops by itself!). I also believe that a drainage tube in most cases will decrease pain and swelling by allowing the collected blood to escape after the surgery. We are designing a home based “self directed ” rehabe program that will allow many total knee patients to avoid the hassles and inconvenience of so many therapy visits. Every patient is different, so we customize the rehab program to the patients needs.
Patients enjoy the improved flexion of modern total knees!
Using a spinal anesthesia also greatly reduces the mental perception of pain, and as the pain returns gradually after surgery, it allows the mind time to accommodate to the pain by and generating the body’s own endorphins ( morhpine like substance that your body creates when it senses trauma or pain). The spinal anesthesia is SAFER than a general anesthesia, because you continue to breathe on your own, without the need for paralytic medications and a machine to breathe for you through a tube. The bottom line is – there is more to the success of a knee replacement then the surgery itself. You need to find a qualified expert – just like you would for any important procedure you might want to have done – Ask your surgeon if he has done a Joint Replacement Fellowship, and how many joints a year he does. Expert total knee surgeons will do over 100 procedures a year, and their results have been shown to be better ( practice makes perfect! ). Dr. Kozinn has been doing 200 to 300 total knees a year for over 20 years – and that is called : EXPERIENCE
Platelet-Rich Plasma (PRP) for knee arthritis.
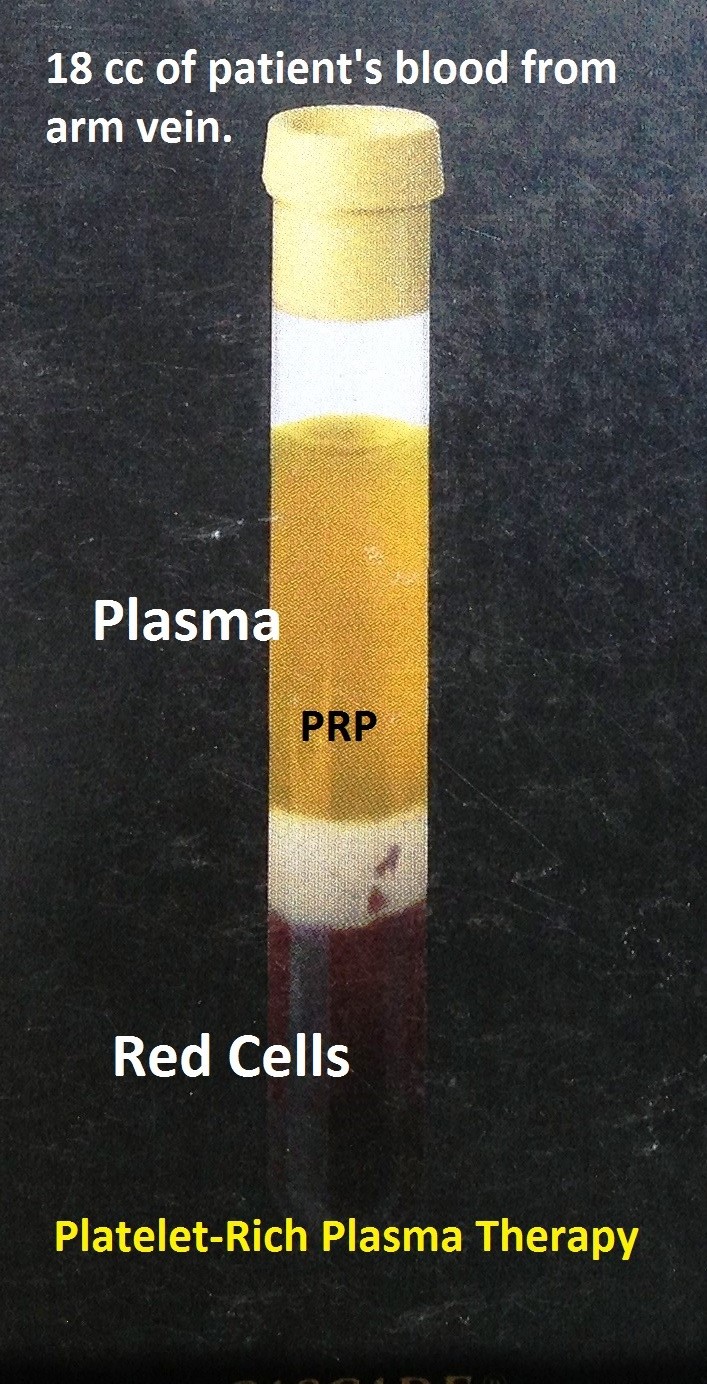
Researchers are always looking for alternatives to cure or treat the symptoms of knee arthritis without resorting to a full knee replacement. Animal studies are on-going to see if embryonic stem cells can regenerate or grow cartilage to replace the worn out cells in an arthritic knee. Another avenue being looked at is Platelet-Rich Plasma (or PRP). Plasma is the golden liquid left over that floats to the top after venous blood is spun down in a high speed centrifuge machine.
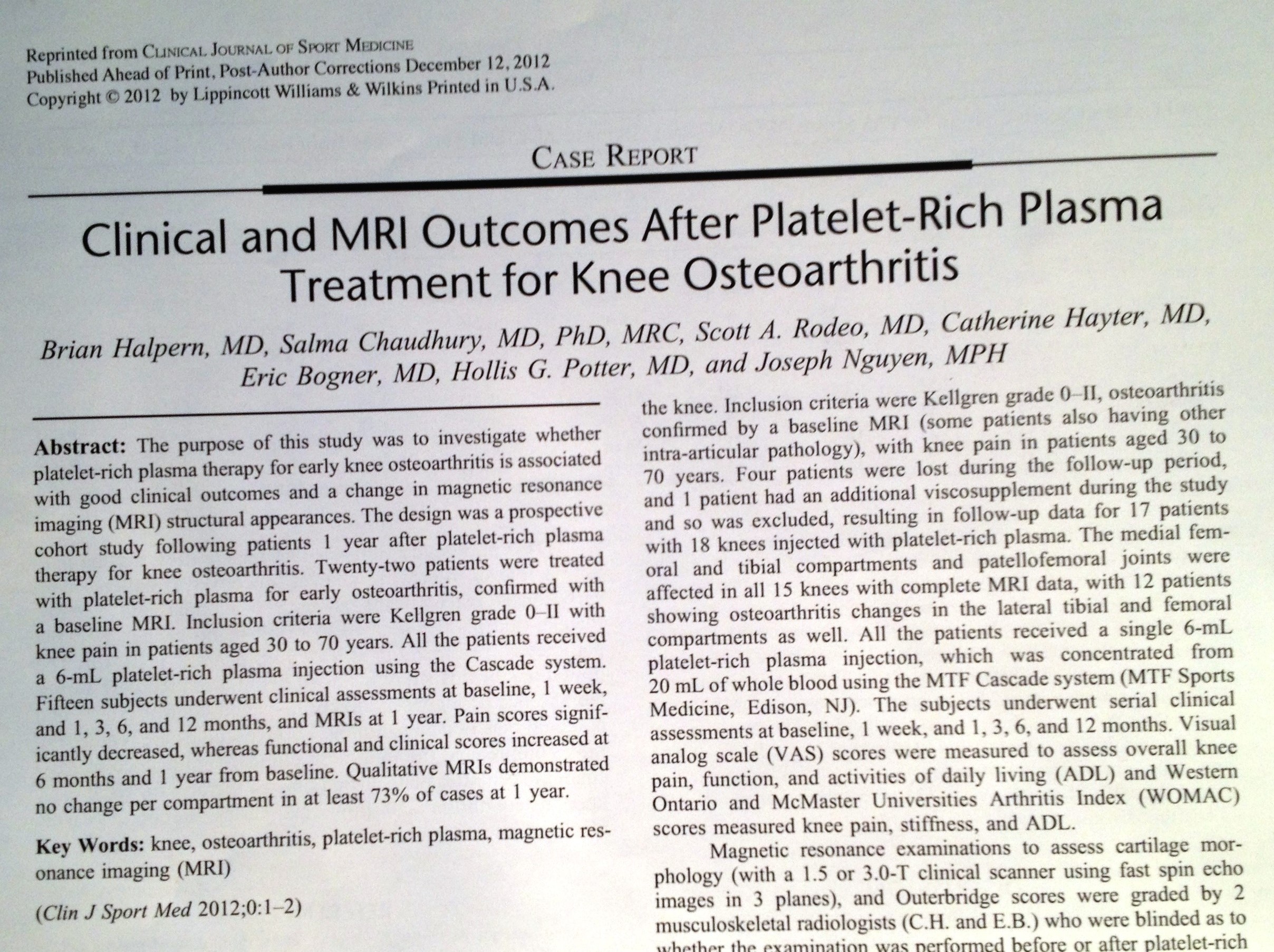
The heavy red blood cells precipitate to the bottom of the tube. In the “old days”, Plasma was used as a blood replacement for trauma or military critical care injuries because it could be frozen and lasted longer than “whole blood”, which has a shorter “shelf life”. many lives were saved by IV infusion of plasma. So it is somewhat ironic that PRP has resurfaced as an exciting new therapy for arthritic knees. The results are not fabulous, but many patients did get relief in a study published in 2012 by The hospital for Special Surgery ( see report below).
The plasma can be prepared from the patients own blood in the doctors office, which is spun down, and the plasma is sterily injected into the patients knee. Simple! The procedure is still considered experimental by insurance carriers, so if you want it done, be prepared to pay for it outside of your insurance coverage!