As imperfect human beings, we are always looking for a way that technology can make us more accurate at what we do. Total knee replacement technology is no different. Unfortunately, every individual and every knee has its own unique “personality” that does not lend itself well to generalized solutions. After working with computer navigation which was the “next big advance” about 10 years ago, we were all disappointed that the overall results of knee replacement were not improved, and in some studies were made worse. We also went through the “phase” of tiny incision “minimally invasive” knee arthroplasty. Results in this group were definitely worse. Part of the reason is the knee has to be perfectly “balanced” through an infinite range of motions and positions. Not just flexion and extension from 0 to 135 degrees, but a variety of rotational positions and “varus-valgus” positions ( side tilt in either direction ). Our computers also can only give us out information based on the “input data” we program into it. If you use “eye-sight” points of information, you will get errors entered into the computer that can easily add up to a worse result than a “free-hand” arthroplasty. It turns out that a trained knee surgeon, after years of practice, has developed a very accurate computer in his (or her) brain. When an external computer is available that is better than my brain, I will switch to it!

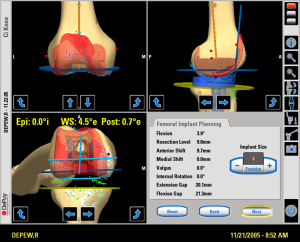
Computer navigation screen for total knee replacement.
Pre-operative CTT scans and MRIs give the computer data in only one knee position! How can the computer know what directions to give the surgeon to make a bone cut in a different position, for instance 90 degrees opposed. It “estimates” based on a data base collected from human volunteers. Also, the computer can not fathom the elasticity, or stretch, in any one person’s ligaments. Since ligament tension is also dependent on the amount of knee flexion, even perfectly directed “bone cuts” can end up with an unstable knee at times because the ligaments must also be under equal tension in all positions. Very hard to accomplish! This is why most high volume total knee surgeons use the “feel” of the knee in their hands as the input to the “computer” in their brains. We “trial” a number of different implant positions and sizes until we get the best and most balanced knee.


Dr. Kozinn with an early version of the Total Knee computer.
The “robots” that are coming out are not better. They have been used for their “marketing value”, as it is natural to assume a robot or computer is “smarter” than a human. Most of the computers out there now still require a human to “manually over-ride” as soon as it is clear that the “pre-set” plan generated from a uni-position CTT or MRI is not going to work out in the real world. A number of research studies have now shown that the surgeon will “abandon” the computerized plan, or revise the cuts yielded from customized cutting blocks up to 70% of the time they are used. Wow! There is also an additional expense and inconvenience of getting these special scans pre-op. I call these custom cutting block operations “total knees by numbers”, analogous to the childhood art game of “paint by numbers”. If you survey most of the high volume fellowship trained total knee surgeons in practice right now, you will find that most do not utilize these devices. When these technologies are really better for patients, we will use them. Right now, it is best to choose an experienced surgeon and not the best robot!
Stuart C. Kozinn MD
Chief of Surgery, HonorHealth Osborn
www.scottsdalejointcenter.com